

Good Reasons for Bad Feelings
Good Reasons for Bad Feelings
A Book Review

The first two years of medical school is a firehose of content, and there’s only a few ways to organize it. MS1 traditionally covers “how the body works” with anatomy and physiology, while MS2 gets to “how things go wrong and what to do about it” with pathology, microbiology, and pharmacology. The alternative is a systems-based approach where, for example, a GI/digestive block covers the structure, function, disorders, and treatments of the GI tract. It’s the same content, sliced differently.
Psychiatry might be included in Neuroscience or kept as a side-dish to the main courses. Either way, the basic psychiatry curriculum covers the DSM categories and symptom criteria, some epidemiology, a heavy dose of pharmacology, and (still) lectures on psychodynamic concepts.
It took me until the 3rd year of residency to realize what’s missing: any sort of psychiatric physiology. Physicians, including psychiatrists, learn almost nothing about the normal function of the brain pertaining to emotions, personality, or any behavior more complex than walking upright.
This isn’t really the fault of medical schools. As Randy Nesse points out, “the core problem for psychiatric diagnosis is the lack of a perspective on normal useful functions that physiology provides for the rest of medicine.” I feel very strongly this is true.
Nesse, a psychiatrist, has been writing about evolutionary psychiatry since 1990, and Good Reasons for Bad Feelings (2019) is the capstone of his academic career. It’srecommended for anyone at all interested in the topic. That said, it reads as almost two books. One is an insightful functionalist approach to common issues like anxiety, mood, and psychosis. The second, less successful, book rehashes well-worn evo psych ideas and falls prey at times to the “just-so story” trap.
I’ll start by briefly summarizing several of his more compelling ideas.
But first, a familiar critique
Like many psychiatrists, Nesse can’t quite conceal his disdain for the DSM. While supposedly agnostic on causes and mechanisms, the DSM implicitly adopts a reductionist view of mental illness as medicalized “brain diseases.” He rounds up various ways this paradigm has failed:
The leading psychiatry textbook says “there is little reason to believe these [DSM] diagnostic categories are valid.”
The NIMH abandoned DSM diagnoses as a basis for research around 2013.
“Brain scans and autopsy studies have identified only small differences” in people with severe mental illness while “there are no common genetic variations with large effects”
Patients receive multiple diagnoses (“comorbidity”) yet those with the same condition can have very different symptoms (“heterogeneity”). There are 227 ways to meet criteria for a diagnosis of MDD.
Boundaries between normal and abnormal are essentially arbitrary.
The DSM encourages a fundamental fallacy: Viewing Symptoms as Diseases.
Nesse is fed up. It’s past time “to ask why specific physical causes for mental disorders are so elusive compared to those for other medical disorders.”
Evolution doesn’t care if you’re happy
Natural selection favors behaviors that maximize reproductive success, not happiness. Negative emotions, as with pain and fever, are unpleasant but often useful. These ideas alone explain most of human misery. But beware a second fallacy, Viewing Diseases as Adaptations: “diseases themselves do not have evolutionary explanations…proposals about the utility of disease are wrong before they start.”
We should try to understand not just disease, but why we have traits that leave us vulnerable to disease. There are six categories of explanation:
Mismatch: our bodies are unprepared to cope with modern environments
Infection: pathogens evolve faster than we do
Constraints: there are some things that natural selection just can’t do
Trade-Offs: every trait has advantages and disadvantages
Reproduction: natural selection maximizes gene replication, not health or happiness
Defensive responses: Adaptive reactions are often unpleasant
The natural focus of a psychiatric physiology is emotions, but…
The scientific study of emotions began in earnest with William James, yet to this day psychologists and neuroscientists can’t agree on definitions for emotion, feeling, mood or affect, much less their mechanisms. Careers have been spent counting up emotions and ascribing a purpose to each. But “each emotion has many functions, and many functions are served by multiple emotions.”

Moreover, emotions aren’t programs designed to clear specification, but evolved “modes of operation that increase ability to cope with certain situations.” They’re like different genre settings on a piano keyboard: big band, marimba, rock ballad. Efforts to tabulate emotions are misguided: like New Wave vs Glam vs Pub Rock, they are distinct only to the extent they differentiated from a common ancestor:

Signal and Noise
It’s commonly taught that anxiety disorders are twice as common in women as men. This depends on the premise that anxiety is bad, and therefore something is wrong with women, their bodies, or society. Flipping the burden, Nesse argues that women have the correct amount of anxiety for their own welfare, while men’s lower average anxiety is dangerous but well-suited for gene transmission.

Even among men, the anxiety distribution is asymmetric due to the “Smoke Detector Principle.” Put simply, protective responses like anxiety (or cough, or pain) skew heavily toward false-positives. A needless panic attack is unpleasant, a false-negative is a genetic dead-end. The ratio of useful fear to pointless fear depends as much on the environment as it does on individual traits.

If your home’s smoke detector was a self-adaptive control system, every burned toast would lower the threshold for the next alert, leading to a cascade of false alarms and an uninhabitable house. This is Panic Disorder and PTSD.
A theory of normal mood is necessary to understand depression or mania.
The universal capacity for something called “mood” needs explanation. We always have one, even if it’s “meh.” Peoples’ moods differ in set point, responsiveness, and amplitude - hallmarks of a regulated control system, which only evolve for important variables like blood glucose, heart rate, or hormone levels. The states we call good (high) and bad (low) mood must somehow be adaptive.
Nesse defines high mood as the “pleasurable state of enthusiasm, energy and optimistic activity associated with situations where activity is likely to pay off grandly,” while low mood is “the painful state of demoralization, low energy, pessimism, risk avoidance, and social withdrawal aroused by situations in which efforts to reach a goal are failing.”
In this model, mood is a mechanism for adjusting effort to match the “propitiousness” of the environment. As a general goal pursuit system, it’s equally applicable to foraging for berries, cultivating friendships, or playing videogames. A context with high payoff per unit investment entails high mood, while low payoff per investment leads to low mood.
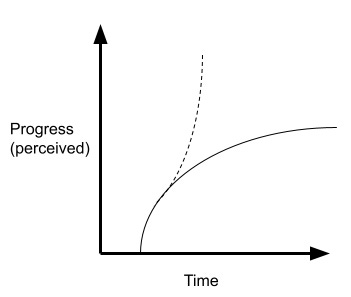
Nesse sees mood as part of the explore-exploit tradeoff, or Charnov’s Marginal Value Theorem. In particular, mood is proportional to the slope (first derivative) of the resource intake function. The subjective experience of mood is “how you know” when to jump on an opportunity, then move on when it’s no longer worth your time.

Sustained low mood, sometimes called depression, is very often a normal response to pursuing unreachable goals. This doesn’t require a brain disorder or dysregulation. Human society, after all, consists of innumerable activities with “huge payoffs for a few winners and years of useless effort for everyone else.”
“Mood disorders result when the moodostat fails”
Mood is a self-adaptive control system. Here are six ways that such systems go awry:
Baseline is too low
Baseline is too high
Response is deficient
Response is excessive
Response is aroused by inappropriate cues
Response is independent of cues
While the failure modes are symmetric, people certainly seem “down” more often than “up.” Low mood, and consequently under-reacting to events, is a low variance strategy that may very well lead to better average outcomes. Life history plays a role as well: repeated failures reflect an adverse environment in which low mood makes sense.
The extremes of high and low mood, in contrast, are not subtle responses to the vagaries of life. Mania and psychotic depression can only reflect a broken “moodostat” that allows runaway positive feedback. Normal people pull back as progress slows, but those prone to mania ignore the cues and redouble their efforts.
Cliff-edge Fitness Landscapes
Schizophrenia, bipolar disorder, and autism are severe illnesses with striking commonalities:
a stable prevalence of ~1% worldwide (with more common milder forms)
large genetic/heritable component
apparently due to tiny effects from a vast number of genes
disastrous for individual function and reproductive success
Why hasn’t natural selection eliminated these diseases?
One explanation, plausible but unsatisfying, is that each disorder results from the accumulation of various new mutations which are only slowly selected against. These aren’t distinct disease entities, but common failure modes due to any number of dysfunctions.
However, the persistence of these conditions in the face of huge fitness costs suggests some selective advantage. How could this work? Most traits follow a normal distribution, with maximal fitness in the middle and poor outcomes at the extremes. The immune system is a good example: people with either extremely weak or strong immune responses tend to do poorly.
But for some traits, fitness is heavily left skewed: increasingly adaptive right up to a “cliff” when it turns catastrophic.
In humans, “strong selection for extreme mental capacities may have given us all minds like the legs of a racehorse, fast but vulnerable to catastrophic failure.” This fits nicely with speculation about schizophrenia and autism emerging out of rapidly expanding human capacities for language, theory of mind, and other cognitive advances.
Critiques
Good Reasons for Bad Feelings has three weaknesses that blunt its otherwise incisive arguments.
First, the core premise of the book, namely that emotions are evolved traits, is more asserted than argued. This point is not universally accepted! Nesse is writing for a lay audience, so I understand his decision to largely avoid neuroscience. However, any reader coming from a more constructivist mindset would not be convinced. Nesse explicitly side-steps any discussion of how emotions might work at a mechanistic level - this is ironic since he identifies the lack of a coherent “physiology” as the central failure of modern psychiatry. Some discussion of the popular works of Fran de Waal, Antonio Damasio, and Jaak Panksepp could go a long way.
Second, despite his criticism of the DSM, Nesse basically adopts its categories and diagnoses as an organizing structure. The book is divided into chapters on anxiety, mood, substance use, eating disorders, and so on. He offers analyses of DSM-defined entities such as panic disorder, MDD, and schizophrenia while elsewhere acknowledging their arbitrary and imprecise nature.
Third, in several places, Nesse provides a run-down of evolutionary explanations for a trait. Low mood could be a “conservation-withdrawal” mode adopted by animals separated from their conspecifics. It could be a generalized help signal, an impetus to reassess social strategies, a self-protective display of social submission, or “deceiving down” to hide one’s abilities and avoid threatening your superiors. Such hypotheses are plausible and fun, but they veer close to the “just-so story” mode of evolutionary explanation. This sort of idea is far more convincing when grounded in neuroscience and ethology, or at least a well-developed model.
Conclusion
Good Reasons for Bad Feelings outlines an approach to mental illness that would undoubtedly improve on psychiatry’s status quo. Nesse has an amiable style with plentiful anecdotes and vignettes. As an introduction to evolutionary psychiatry, it’s far more approachable than comparable works by del Giudice and Brune.
So, is neo-Darwinian evolution the best framework for understanding mental illness? I’m less sure. Explanations of human (animal!) behavior and neuroscience must be constrained by the reality of evolution, but analyzing specific phenomena in this mode strikes me as its own form of reductionism. Moreover, without a clear model, you still face a “missing middle” problem that allows just-so stories to flourish.

Nesse correctly identifies a lack of a coherent “physiology” as the core problem in psychiatry. In other words, we still lack good explanations compared to the rest of medicine. This failure is partly due to the brain’s complexity, but psychiatrists all too often enable bad explanations for mental illness to persist: see psychoanalysis, chemical imbalances, genetic markers. The subjective, symptom to syndrome paradigm of the DSM will not help us here. Nesse strives for better explanations, and mostly succeeds.